3例涎腺癌肉瘤的临床诊疗分析
时间:2018-09-03 来源:诊断病理学杂志 作者:白玉萍,岳常丽,张勇 本文字数:6059字
摘 要:目的 探讨涎腺癌肉瘤的临床病理特点, 加深对该肿瘤的认识。方法 回顾性分析3例涎腺癌肉瘤的临床病理资料, 并进行随访。结果 3例中男性2例, 女性1例。年龄6668岁, 平均年龄67岁, 中位年龄67岁。2例以无痛性肿物就诊, 1例肿物伴疼痛。3例分别发生于右侧腮腺、左侧颌下腺及右侧咽旁间隙。均无涎腺多形性腺瘤病史。组织学上, 3例中1例以肉瘤为主, 1例以癌为主, 1例肉瘤与癌比例相当。肉瘤成分, 2例为平滑肌肉瘤, 1例为纤维肉瘤;癌成分, 3例均包括导管癌和鳞状细胞癌, 其中1例还包括少量未分化癌。3例肿瘤中均未发现多形性腺瘤成分。免疫组化:肉瘤成分vimentin均 (+) , 癌成分CK均 (+) ;导管癌AR均 (+) .3例中1例肉瘤成分与未分化癌成分呈CK和vimentin双 (+) .随访2例, 随访时间35个月, 未出现复发及转移。失访1例。结论 涎腺癌肉瘤发病罕见, 确诊需依靠组织病理检查, 免疫组化染色有助诊断。文献表明该肿瘤恶性程度高, 预后差, 需长期随访。

关键词:涎腺; 癌肉瘤; 病理学;
Abstract: Objective To investigate the clinicopathological features of carcinosarcoma of salivary glands in order to increase awareness of this entity.Methods The clinicopathological data of 3 cases of salivary carcinosarcoma were retrospectively analyzed.The prognosis of 2 patients was followed up.Results The 3 cases of salivary adenocarcinoma occurred in the right parotid gland, the left submandibular gland and the right pharyngeal space respectively.Patients were2 males and 1 female ( mean age, 67 years;median age, 67 years;range, 66-68 years) .Two patients presented with a painless mass, and the other one with a painful mass.None of them had history of salivary adenomatous adenomas.Histologically, one case of tumor was composed predominantly of sarcoma, one was composed predominantly of carcinoma, and there were roughly equal sarcomatous and carcinomatous components in the other one.As for the type of sarcomatous components, 2 cases were leiomyosarcoma and one was fibrosarcoma.The carcinomatous components consisted of ductal adenocarcinoma and squamous cell carcinoma in 2 of 3 cases.Ductal adenocarcinoma, squamous cell carcinoma and a small amount of undifferentiated carcinoma component were noted in the other case of tumor.No pleomorphic adenoma was detected in 3 of the tumors.Immunohistochemically, the sarcomatous component was positive for vimentin in all the cases, the cancerous component was positive for cytokeratin in all the cases, ductal carcinoma was positive for AR in all the cases.In 1 of the 3 cases, both the sarcomatous component and the undifferentiated carcinoma were positive for both cytokeratin and vimentin.Neither local recurence nor metastasis was detected in 2 patients during 3 ~ 5 months follow-up.One case was lost.Conclusion Carcinosarcoma of salivary is a rare malignant tumor.Conformation of the diagnosis relies on histopathological examination.Immunohistochemical staining is assistant for the diagnosis.The literature indicates that this tumor is a high-grade malignant tumor with poor prognosis, and therefore long-term follow-up is recommended for these patients.
Keyword: Salivary; Carcinosarcoma; Pathology;
首例涎腺癌肉瘤报道于1951年[1].该肿瘤极为罕见, 迄今为止, 国内文献报道仅10例。我们收集3例涎腺癌肉瘤的临床病理资料进行观察、分析, 并复习了相关文献, 以期加深对该肿瘤的认识。
1、 材料与方法
1.1、 材料
收集首都医科大学附属北京同仁医院2011-05-2017-08间3例涎腺癌肉瘤的临床及病理资料。3例均为首次发病就诊。男性2例, 女性1例。发病年龄66~68岁, 平均年龄67岁, 中位年龄67岁。肿瘤分别发生于右侧腮腺、左侧颌下腺及右侧咽旁间隙。2例为无痛性肿物, 1例肿物伴疼痛。2例行MRI检查显示肿物边界不清, 提示恶性病变, 1例行超声检查, 未提示肿物性质。3例均行肿物切除 (表1) .
1.2、 方法
标本均经4%的甲醛固定, 石蜡包埋, 4μm厚切片, HE染色, 光镜下观察。免疫组化采用En Vision二步法。DAB显色。一抗抗体p40、CK8/18、AR、SMA、MSA、calponin、CD34、bcl-2、S-100和Ki-67均购自北京中杉金桥生物技术有限公司。
2、 结果
2.1、 巨检
3例肿瘤均为灰白、灰黄色实性结节状肿物, 质地中~韧, 肿瘤边界欠清。
2.2、 镜检
3例镜下均由恶性上皮性成分 (癌) 和恶性间叶性成分 (肉瘤) 构成, 两种成分相互混杂。
例1, 肿瘤以癌为主, 可见片状坏死区。肉瘤成分为纤维肉瘤, 梭形瘤细胞呈束状、编织状排列, 核呈中、高度异型性 (图1, 2) .例2, 肿瘤中癌与肉瘤比例相当, 可见片状坏死区。肉瘤成分为平滑肌肉瘤, 梭形瘤细胞呈编织状、束状排列, 核呈中度异型性 (图3) .例3, 肿瘤以肉瘤为主, 可见灶状坏死区。肉瘤成分为平滑肌肉瘤, 梭形瘤细胞呈编织状、束状排列 (图4, 5) , 核呈中、高度异型性 (表2) .
2.3、 免疫组化
3例癌成分均CK (+) , 肉瘤成分均vimentin (+) .部分导管癌巢周可见肌上皮细胞p63和calponin (+) .
例1, 肉瘤成分SMA、calponin、CD34、bcl-2、S-100和p63 (-) , Ki-67增殖指数75%.癌组织为主要成分, 包括低分化导管癌和鳞状细胞癌, 以导管癌为主, 仅见少量鳞状细胞癌。导管癌CK8/18、AR和PAS (+) , 鳞状细胞癌p63和p40 (+) (图6, 7) .例2, 肉瘤成分SMA、calponin (+) , CD34、bcl-2、S-100和p63 (-) , Ki-67指数约10%.癌包括低分化导管癌和不同分化程度的鳞状细胞癌, 两者比例相当;导管癌AR (图8) 、CK8/18和PAS (+) , 鳞状细胞癌p63和p40 (+) .例3, 肉瘤成分SMA、MSA和calponin (+) , CD34、bcl-2、S-100和p63 (-) , Ki-67指数约30%.癌为次要成分, 包括中-低分化鳞状细胞癌和中分化导管癌、未分化癌, 其中以鳞状细胞癌为主;导管癌AR (图8) 、CK8/18和PAS (+) , 鳞状细胞癌p63和p40 (+) .本例中, 肉瘤组织与未分化癌组织呈CK和vimentin双 (+) .
病理诊断:癌肉瘤。
例1肿瘤发生右侧颈部淋巴结多发转移 (5/5) , 多处脉管可见瘤栓。例2、例3肿瘤未发生淋巴结转移。例3手术联合放疗, 随访5个月, 目前情况良好, 未出现复发及转移。例2术后未行放、化疗, 随访3个月, 目前情况良好, 未出现复发及转移。例1失访。
3、 讨论
涎腺癌肉瘤也称真性恶性混合瘤, 是一种罕见的恶性侵袭性肿瘤。由于该肿瘤罕见, 目前对其认识尚存不足。

图1例1, 导管癌 (右) 与肉瘤 (左) 混合区图2例1, 肉瘤与鳞状细胞癌混合区图3例2, 低分化导管癌图4例3, 肉瘤区, 梭形细胞呈编织状、束状排列图5例3, 导管癌图6例1, 癌CK (+) , 肉瘤CK (-) En Vision法图7例1, 肉瘤vimentin (+) , 癌vimentin (-) En Vision法图8例2, 低分化导管癌AR (+) En Vision法
涎腺癌肉瘤占所有涎腺肿瘤的0.04%~0.16%, 占涎腺恶性肿瘤的0.4%[2].约65%发生于腮腺[3].患者通常60~65岁, 多数报告没有性别差异[3].通常表现为肿块, 可伴疼痛, 发生于腮腺者可伴有面神经麻痹等。本组3例, 1例发生于腮腺, 1例发生于颌下腺, 1例发生于咽旁间隙。3例年龄分别为66、67和68岁, 与报道相符。2例因无痛性肿物就诊, 1例肿物伴疼痛。涎腺癌肉瘤可发生于既存的多形性腺瘤也可为原发性。本组3例均无涎腺多形性腺瘤病史, 肿瘤经充分取材亦未发现多形性腺瘤成分, 故3例均为原发性涎腺癌肉瘤。影像学检查对涎腺癌肉瘤具有提示恶性作用[4].3例中2例影像学检查提示为恶性。确诊该肿瘤需行病理检查。
3.1、 诊断
大体观察, 涎腺癌肉瘤为灰白、灰黄色实性肿物, 因肿瘤具有侵袭性而至边界模糊。镜下, 涎腺癌肉瘤为双相性, 由不同比例的恶性上皮性成分 (癌) 和恶性间叶性成分 (肉瘤) 构成。癌最常见的类型是鳞状细胞癌、腺癌和未分化癌;肉瘤以软骨肉瘤、纤维肉瘤、平滑肌肉瘤、骨肉瘤以及脂肪肉瘤最常见[5].本组3例, 肉瘤成分2例为平滑肌肉瘤, 1例为纤维肉瘤。癌成分均包括导管癌和鳞状细胞癌, 3例中1例还包括少量未分化癌。文献报告中涎腺癌肉瘤的癌类型还包括黏液表皮样癌[6]、大细胞神经内分泌癌[7];肉瘤类型还包括横纹肌肉瘤[5、7、8]、恶性纤维组织细胞瘤[9]/多形性未分化肉瘤[10]、滤泡树突细胞肉瘤[11].癌成分CK阳性, 肉瘤成分vimentin阳性, 支持癌肉瘤诊断;而AR、CK8/18和PAS阳性有助于导管癌诊断, 尤其AR具有较高的特异性。p63、p40和CK5/6阳性有助于鳞状细胞癌诊断。
3.2、 鉴别诊断
涎腺癌肉瘤需与更为常见的癌在多形性腺瘤中和单纯的涎腺肉瘤鉴别。癌在多形性腺瘤中的其他成分为良性, 而单纯的涎腺肉瘤没有上皮成分。涎腺癌肉瘤的肉瘤成分为弥漫梭形细胞时还需与梭形细胞肌上皮癌鉴别。肌上皮癌可见小的鳞状上皮分化区, 罕见情况下也可见导管样腔隙。肌上皮癌CK、p63常弥漫阳性, 有助于二者的区分。文献报告腮腺癌肉瘤胸膜转移可能会被误诊为间皮瘤[12].癌肉瘤和间皮瘤均为双相性肿瘤, 对有癌肉瘤病史的患者发现胸膜占位应首先考虑癌肉瘤转移的可能。文献报告皮肤癌肉瘤可转移至腮腺[13], 对有其他部位癌肉瘤病史的患者发现涎腺癌肉瘤应考虑到转移灶的可能。涎腺癌肉瘤还应与转移性多形性腺瘤鉴别。该瘤亦罕见, 但原发和转移病灶内的上皮和间质成分组织学上均呈良性表现。
3.3、 起源
涎腺癌肉瘤的细胞起源尚不明确, 目前较统一的观点认为该肿瘤可能起源于肌上皮细胞。Vékony等[14]对1例腮腺癌肉瘤行寡核苷酸阵列比较基因组杂交 (CGH) 检测, 发现上皮和间质成分显示相似的基因组图谱, 癌成分与肉瘤成分基因组图谱的整体同源性是75%, 提示二者为单克隆起源。Vélez-Pérez等[15]对1例腮腺癌肉瘤进行了蛋白质组学分析, 结果显示癌与肉瘤成分表达上皮-间质转化相关标记物 (SPARC、Gli2和p-STAT3[Tyr705]) .这一发现也提示涎腺癌肉瘤的癌与肉瘤成分为单克隆起源。G9tte等[16]对1例免疫组化染色显示SMA阴性的腮腺癌肉瘤进行电镜分析, 检测到了胞质肌上皮结构。这一结果支持涎腺癌肉瘤的单克隆起源假说, 肌上皮细胞是这一共同干细胞最可能的候选。本组3例中1例未分化癌与肉瘤成分呈CK、vimentin双阳性。这一结果也支持癌与肉瘤两种成分的单克隆起源。
3.4、 治疗与预后
外科手术联合术后放疗是涎腺癌肉瘤的标准治疗模式[17].该肿瘤的侵袭性非常强, 高达50%的患者出现局部复发和局部及区域性转移[2], 54%的患者发生远处转移[3].约1/3原发性涎腺癌肉瘤患者中位生存期为10个月[18].本组3例均行手术治疗。1例就诊时肿瘤已发生广泛区域性淋巴结转移, 术后失访。另2例随访时间较短 (3~5个月) , 其中1例行术后放疗, 随访期间2例均未复发和转移。因该肿瘤恶性程度高, 易于复发和转移, 需长期随访。
参考文献:
[1]Kirklin JW, Mc Donald JR, Harrington SW, et al.Parotid tumors:histopathology, clinical behaviour and end results[J].Surg Gynecol Obstet, 1951, 92 (6) :721-733.
[2]Gnepp DR.Malignant mixed tumors of the salivary glands:a review[J].Pathol Annu, 1993, 28 (1) :279-328.
[3]Phan HNM, Hong YT, Hong KH.Primary carcinosarcoma of the parotid gland mimicking as parotid abscess with deep neck infection[J].J Craniofac Surg, 2017, 28 (3) :e210-e213.
[4]Fan KF, Connor SE, Macbean AD, et al.MRI findings of carcinosarcoma in the parotid gland[J].Oral Oncol, 2006, 42 (3) :323-326.
[5]Kwon MY, Gu M.True malignant mixed tumor (carcinosarcoma) of parotid gland with unusual mesenchymal component:a case report and review of the literature[J].Arch Pathol Lab Med, 2001, 125 (6) :812-815.
[6]张海萍, 张海芳, 陈培琼。腮腺癌肉瘤一例[J].中华病理学杂志, 2011, 40 (10) :703-704.
[7]Ueo T, Kaku N, Kashima K, et al.Carcinosarcoma of the parotid gland:an unusual case with large-cell neuroendocrine carcinoma and rhabdomyosarcoma[J].APMIS, 2005, 113 (6) :456-464.
[8]Gandour-Edwards RF, Donald PJ, Vogt PJ, et al.Carcinosarcoma (malignant mixed tumor) of the parotid:report of a case with a pure rhabdomyosarcoma component[J].Head Neck, 1994, 16 (4) :379-382.
[9]Latkovich P, Johnson RL.Carcinosarcoma of the parotid gland:report of a case with cytohistologic and immunohistochemical findings[J].Arch Pathol Lab Med, 1998, 122 (8) :743-746.
[10]Manuel S, Mathews A, Chandramohan K, et al.Carcinosarcoma of the parotid gland with epithelial-myoepithelial carcinoma and pleomorphic sarcoma components[J].Br J Oral Maxillofac Surg, 2002, 40 (6) :480-483.
[11]Liu Q, Zhu JS, Xu YP.Parotid gland carcinosarcoma with follicular dendritic cell sarcoma as mesenchymal component:a case report[J].Chin Med J (Engl) , 2005, 20;118 (6) :516-518.
[12]Khadse P, Prabhash K, Pramesh CS, et al.Fine-needle aspiration biopsy of pleural metastases from a carcinosarcoma or true malignant mixed tumor of the parotid gland mimicking a mesothelioma[J].Diagn Cytopathol, 2009, 37 (9) :680-685.
[13]Loh TL, Tomlinson J, Chin R, et al.Cutaneous carcinosarcoma with metastasis to the parotid gland[J].Case Rep Otolaryngol, 2014, 2014:173235.
[14]Vékony H, Leemans CR, Ylstra B, et al.Salivary gland carcinosarcoma:oligonucleotide array CGH reveals similar genomic profiles in epithelial and mesenchymal components[J].Oral Oncol, 2009, 45 (3) :259-265.
[15]Vélez-Pérez A, Huang RS, Everett JM, et al.Carcinosarcoma of the parotid:investigating its biology with morphoproteomics[J].Int J Surg Pathol, 2015, 23 (2) :116-121.
[16]G9tte K, Riedel F, Coy JF, et al.Salivary gland carcinosarcoma:immunohistochemical, molecular genetic and electron microscopic findings[J].Oral Oncol, 2000, 36 (4) :360-364.
[17]Taki NH, Laver N, Quinto T, et al.Carcinosarcoma de novo of the parotid gland:case report[J].Head Neck, 2013, 35 (5) :E161-E163.
[18]Staffieri C, Marioni G, Ferraro SM, et al.Carcinosarcoma de novo of the parotid gland[J].Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2007, 104 (2) :e35-40.
Abstract: Objective To investigate the clinicopathological features of carcinosarcoma of salivary glands in order to increase awareness of this entity.Methods The clinicopathological data of 3 cases of salivary carcinosarcoma were retrospectively analyzed.The prognosis of 2 patients was followed up.Results The 3 cases of salivary adenocarcinoma occurred in the right parotid gland, the left submandibular gland and the right pharyngeal space respectively.Patients were2 males and 1 female ( mean age, 67 years;median age, 67 years;range, 66-68 years) .Two patients presented with a painless mass, and the other one with a painful mass.None of them had history of salivary adenomatous adenomas.Histologically, one case of tumor was composed predominantly of sarcoma, one was composed predominantly of carcinoma, and there were roughly equal sarcomatous and carcinomatous components in the other one.As for the type of sarcomatous components, 2 cases were leiomyosarcoma and one was fibrosarcoma.The carcinomatous components consisted of ductal adenocarcinoma and squamous cell carcinoma in 2 of 3 cases.Ductal adenocarcinoma, squamous cell carcinoma and a small amount of undifferentiated carcinoma component were noted in the other case of tumor.No pleomorphic adenoma was detected in 3 of the tumors.Immunohistochemically, the sarcomatous component was positive for vimentin in all the cases, the cancerous component was positive for cytokeratin in all the cases, ductal carcinoma was positive for AR in all the cases.In 1 of the 3 cases, both the sarcomatous component and the undifferentiated carcinoma were positive for both cytokeratin and vimentin.Neither local recurence nor metastasis was detected in 2 patients during 3 ~ 5 months follow-up.One case was lost.Conclusion Carcinosarcoma of salivary is a rare malignant tumor.Conformation of the diagnosis relies on histopathological examination.Immunohistochemical staining is assistant for the diagnosis.The literature indicates that this tumor is a high-grade malignant tumor with poor prognosis, and therefore long-term follow-up is recommended for these patients.
Keyword: Salivary; Carcinosarcoma; Pathology;
首例涎腺癌肉瘤报道于1951年[1].该肿瘤极为罕见, 迄今为止, 国内文献报道仅10例。我们收集3例涎腺癌肉瘤的临床病理资料进行观察、分析, 并复习了相关文献, 以期加深对该肿瘤的认识。
1、 材料与方法
1.1、 材料
收集首都医科大学附属北京同仁医院2011-05-2017-08间3例涎腺癌肉瘤的临床及病理资料。3例均为首次发病就诊。男性2例, 女性1例。发病年龄66~68岁, 平均年龄67岁, 中位年龄67岁。肿瘤分别发生于右侧腮腺、左侧颌下腺及右侧咽旁间隙。2例为无痛性肿物, 1例肿物伴疼痛。2例行MRI检查显示肿物边界不清, 提示恶性病变, 1例行超声检查, 未提示肿物性质。3例均行肿物切除 (表1) .
1.2、 方法
标本均经4%的甲醛固定, 石蜡包埋, 4μm厚切片, HE染色, 光镜下观察。免疫组化采用En Vision二步法。DAB显色。一抗抗体p40、CK8/18、AR、SMA、MSA、calponin、CD34、bcl-2、S-100和Ki-67均购自北京中杉金桥生物技术有限公司。
2、 结果
2.1、 巨检
3例肿瘤均为灰白、灰黄色实性结节状肿物, 质地中~韧, 肿瘤边界欠清。
2.2、 镜检
3例镜下均由恶性上皮性成分 (癌) 和恶性间叶性成分 (肉瘤) 构成, 两种成分相互混杂。
例1, 肿瘤以癌为主, 可见片状坏死区。肉瘤成分为纤维肉瘤, 梭形瘤细胞呈束状、编织状排列, 核呈中、高度异型性 (图1, 2) .例2, 肿瘤中癌与肉瘤比例相当, 可见片状坏死区。肉瘤成分为平滑肌肉瘤, 梭形瘤细胞呈编织状、束状排列, 核呈中度异型性 (图3) .例3, 肿瘤以肉瘤为主, 可见灶状坏死区。肉瘤成分为平滑肌肉瘤, 梭形瘤细胞呈编织状、束状排列 (图4, 5) , 核呈中、高度异型性 (表2) .
2.3、 免疫组化
3例癌成分均CK (+) , 肉瘤成分均vimentin (+) .部分导管癌巢周可见肌上皮细胞p63和calponin (+) .
例1, 肉瘤成分SMA、calponin、CD34、bcl-2、S-100和p63 (-) , Ki-67增殖指数75%.癌组织为主要成分, 包括低分化导管癌和鳞状细胞癌, 以导管癌为主, 仅见少量鳞状细胞癌。导管癌CK8/18、AR和PAS (+) , 鳞状细胞癌p63和p40 (+) (图6, 7) .例2, 肉瘤成分SMA、calponin (+) , CD34、bcl-2、S-100和p63 (-) , Ki-67指数约10%.癌包括低分化导管癌和不同分化程度的鳞状细胞癌, 两者比例相当;导管癌AR (图8) 、CK8/18和PAS (+) , 鳞状细胞癌p63和p40 (+) .例3, 肉瘤成分SMA、MSA和calponin (+) , CD34、bcl-2、S-100和p63 (-) , Ki-67指数约30%.癌为次要成分, 包括中-低分化鳞状细胞癌和中分化导管癌、未分化癌, 其中以鳞状细胞癌为主;导管癌AR (图8) 、CK8/18和PAS (+) , 鳞状细胞癌p63和p40 (+) .本例中, 肉瘤组织与未分化癌组织呈CK和vimentin双 (+) .
病理诊断:癌肉瘤。
例1肿瘤发生右侧颈部淋巴结多发转移 (5/5) , 多处脉管可见瘤栓。例2、例3肿瘤未发生淋巴结转移。例3手术联合放疗, 随访5个月, 目前情况良好, 未出现复发及转移。例2术后未行放、化疗, 随访3个月, 目前情况良好, 未出现复发及转移。例1失访。
3、 讨论
涎腺癌肉瘤也称真性恶性混合瘤, 是一种罕见的恶性侵袭性肿瘤。由于该肿瘤罕见, 目前对其认识尚存不足。
表1 3例涎腺癌肉瘤临床资料
表2 3例涎腺癌肉瘤组织学特点
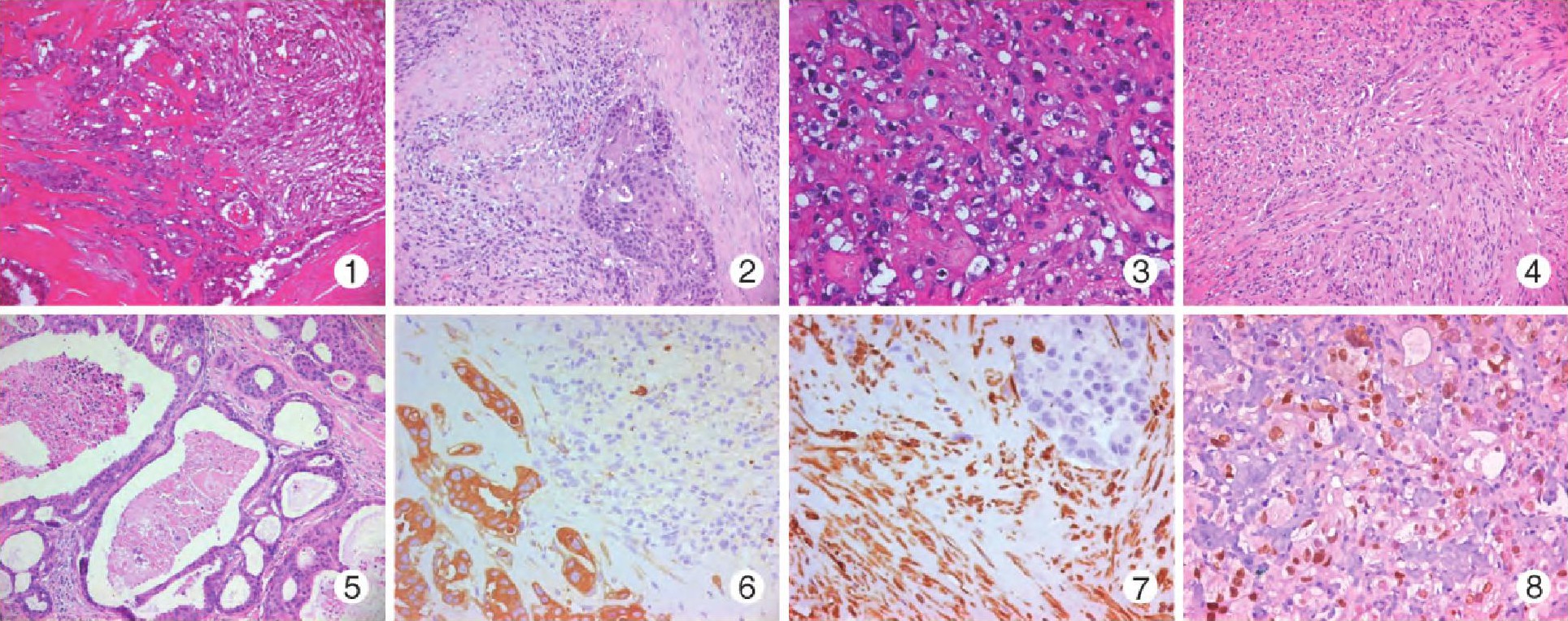
图1例1, 导管癌 (右) 与肉瘤 (左) 混合区图2例1, 肉瘤与鳞状细胞癌混合区图3例2, 低分化导管癌图4例3, 肉瘤区, 梭形细胞呈编织状、束状排列图5例3, 导管癌图6例1, 癌CK (+) , 肉瘤CK (-) En Vision法图7例1, 肉瘤vimentin (+) , 癌vimentin (-) En Vision法图8例2, 低分化导管癌AR (+) En Vision法
涎腺癌肉瘤占所有涎腺肿瘤的0.04%~0.16%, 占涎腺恶性肿瘤的0.4%[2].约65%发生于腮腺[3].患者通常60~65岁, 多数报告没有性别差异[3].通常表现为肿块, 可伴疼痛, 发生于腮腺者可伴有面神经麻痹等。本组3例, 1例发生于腮腺, 1例发生于颌下腺, 1例发生于咽旁间隙。3例年龄分别为66、67和68岁, 与报道相符。2例因无痛性肿物就诊, 1例肿物伴疼痛。涎腺癌肉瘤可发生于既存的多形性腺瘤也可为原发性。本组3例均无涎腺多形性腺瘤病史, 肿瘤经充分取材亦未发现多形性腺瘤成分, 故3例均为原发性涎腺癌肉瘤。影像学检查对涎腺癌肉瘤具有提示恶性作用[4].3例中2例影像学检查提示为恶性。确诊该肿瘤需行病理检查。
3.1、 诊断
大体观察, 涎腺癌肉瘤为灰白、灰黄色实性肿物, 因肿瘤具有侵袭性而至边界模糊。镜下, 涎腺癌肉瘤为双相性, 由不同比例的恶性上皮性成分 (癌) 和恶性间叶性成分 (肉瘤) 构成。癌最常见的类型是鳞状细胞癌、腺癌和未分化癌;肉瘤以软骨肉瘤、纤维肉瘤、平滑肌肉瘤、骨肉瘤以及脂肪肉瘤最常见[5].本组3例, 肉瘤成分2例为平滑肌肉瘤, 1例为纤维肉瘤。癌成分均包括导管癌和鳞状细胞癌, 3例中1例还包括少量未分化癌。文献报告中涎腺癌肉瘤的癌类型还包括黏液表皮样癌[6]、大细胞神经内分泌癌[7];肉瘤类型还包括横纹肌肉瘤[5、7、8]、恶性纤维组织细胞瘤[9]/多形性未分化肉瘤[10]、滤泡树突细胞肉瘤[11].癌成分CK阳性, 肉瘤成分vimentin阳性, 支持癌肉瘤诊断;而AR、CK8/18和PAS阳性有助于导管癌诊断, 尤其AR具有较高的特异性。p63、p40和CK5/6阳性有助于鳞状细胞癌诊断。
3.2、 鉴别诊断
涎腺癌肉瘤需与更为常见的癌在多形性腺瘤中和单纯的涎腺肉瘤鉴别。癌在多形性腺瘤中的其他成分为良性, 而单纯的涎腺肉瘤没有上皮成分。涎腺癌肉瘤的肉瘤成分为弥漫梭形细胞时还需与梭形细胞肌上皮癌鉴别。肌上皮癌可见小的鳞状上皮分化区, 罕见情况下也可见导管样腔隙。肌上皮癌CK、p63常弥漫阳性, 有助于二者的区分。文献报告腮腺癌肉瘤胸膜转移可能会被误诊为间皮瘤[12].癌肉瘤和间皮瘤均为双相性肿瘤, 对有癌肉瘤病史的患者发现胸膜占位应首先考虑癌肉瘤转移的可能。文献报告皮肤癌肉瘤可转移至腮腺[13], 对有其他部位癌肉瘤病史的患者发现涎腺癌肉瘤应考虑到转移灶的可能。涎腺癌肉瘤还应与转移性多形性腺瘤鉴别。该瘤亦罕见, 但原发和转移病灶内的上皮和间质成分组织学上均呈良性表现。
3.3、 起源
涎腺癌肉瘤的细胞起源尚不明确, 目前较统一的观点认为该肿瘤可能起源于肌上皮细胞。Vékony等[14]对1例腮腺癌肉瘤行寡核苷酸阵列比较基因组杂交 (CGH) 检测, 发现上皮和间质成分显示相似的基因组图谱, 癌成分与肉瘤成分基因组图谱的整体同源性是75%, 提示二者为单克隆起源。Vélez-Pérez等[15]对1例腮腺癌肉瘤进行了蛋白质组学分析, 结果显示癌与肉瘤成分表达上皮-间质转化相关标记物 (SPARC、Gli2和p-STAT3[Tyr705]) .这一发现也提示涎腺癌肉瘤的癌与肉瘤成分为单克隆起源。G9tte等[16]对1例免疫组化染色显示SMA阴性的腮腺癌肉瘤进行电镜分析, 检测到了胞质肌上皮结构。这一结果支持涎腺癌肉瘤的单克隆起源假说, 肌上皮细胞是这一共同干细胞最可能的候选。本组3例中1例未分化癌与肉瘤成分呈CK、vimentin双阳性。这一结果也支持癌与肉瘤两种成分的单克隆起源。
3.4、 治疗与预后
外科手术联合术后放疗是涎腺癌肉瘤的标准治疗模式[17].该肿瘤的侵袭性非常强, 高达50%的患者出现局部复发和局部及区域性转移[2], 54%的患者发生远处转移[3].约1/3原发性涎腺癌肉瘤患者中位生存期为10个月[18].本组3例均行手术治疗。1例就诊时肿瘤已发生广泛区域性淋巴结转移, 术后失访。另2例随访时间较短 (3~5个月) , 其中1例行术后放疗, 随访期间2例均未复发和转移。因该肿瘤恶性程度高, 易于复发和转移, 需长期随访。
参考文献:
[1]Kirklin JW, Mc Donald JR, Harrington SW, et al.Parotid tumors:histopathology, clinical behaviour and end results[J].Surg Gynecol Obstet, 1951, 92 (6) :721-733.
[2]Gnepp DR.Malignant mixed tumors of the salivary glands:a review[J].Pathol Annu, 1993, 28 (1) :279-328.
[3]Phan HNM, Hong YT, Hong KH.Primary carcinosarcoma of the parotid gland mimicking as parotid abscess with deep neck infection[J].J Craniofac Surg, 2017, 28 (3) :e210-e213.
[4]Fan KF, Connor SE, Macbean AD, et al.MRI findings of carcinosarcoma in the parotid gland[J].Oral Oncol, 2006, 42 (3) :323-326.
[5]Kwon MY, Gu M.True malignant mixed tumor (carcinosarcoma) of parotid gland with unusual mesenchymal component:a case report and review of the literature[J].Arch Pathol Lab Med, 2001, 125 (6) :812-815.
[6]张海萍, 张海芳, 陈培琼。腮腺癌肉瘤一例[J].中华病理学杂志, 2011, 40 (10) :703-704.
[7]Ueo T, Kaku N, Kashima K, et al.Carcinosarcoma of the parotid gland:an unusual case with large-cell neuroendocrine carcinoma and rhabdomyosarcoma[J].APMIS, 2005, 113 (6) :456-464.
[8]Gandour-Edwards RF, Donald PJ, Vogt PJ, et al.Carcinosarcoma (malignant mixed tumor) of the parotid:report of a case with a pure rhabdomyosarcoma component[J].Head Neck, 1994, 16 (4) :379-382.
[9]Latkovich P, Johnson RL.Carcinosarcoma of the parotid gland:report of a case with cytohistologic and immunohistochemical findings[J].Arch Pathol Lab Med, 1998, 122 (8) :743-746.
[10]Manuel S, Mathews A, Chandramohan K, et al.Carcinosarcoma of the parotid gland with epithelial-myoepithelial carcinoma and pleomorphic sarcoma components[J].Br J Oral Maxillofac Surg, 2002, 40 (6) :480-483.
[11]Liu Q, Zhu JS, Xu YP.Parotid gland carcinosarcoma with follicular dendritic cell sarcoma as mesenchymal component:a case report[J].Chin Med J (Engl) , 2005, 20;118 (6) :516-518.
[12]Khadse P, Prabhash K, Pramesh CS, et al.Fine-needle aspiration biopsy of pleural metastases from a carcinosarcoma or true malignant mixed tumor of the parotid gland mimicking a mesothelioma[J].Diagn Cytopathol, 2009, 37 (9) :680-685.
[13]Loh TL, Tomlinson J, Chin R, et al.Cutaneous carcinosarcoma with metastasis to the parotid gland[J].Case Rep Otolaryngol, 2014, 2014:173235.
[14]Vékony H, Leemans CR, Ylstra B, et al.Salivary gland carcinosarcoma:oligonucleotide array CGH reveals similar genomic profiles in epithelial and mesenchymal components[J].Oral Oncol, 2009, 45 (3) :259-265.
[15]Vélez-Pérez A, Huang RS, Everett JM, et al.Carcinosarcoma of the parotid:investigating its biology with morphoproteomics[J].Int J Surg Pathol, 2015, 23 (2) :116-121.
[16]G9tte K, Riedel F, Coy JF, et al.Salivary gland carcinosarcoma:immunohistochemical, molecular genetic and electron microscopic findings[J].Oral Oncol, 2000, 36 (4) :360-364.
[17]Taki NH, Laver N, Quinto T, et al.Carcinosarcoma de novo of the parotid gland:case report[J].Head Neck, 2013, 35 (5) :E161-E163.
[18]Staffieri C, Marioni G, Ferraro SM, et al.Carcinosarcoma de novo of the parotid gland[J].Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2007, 104 (2) :e35-40.
- 相关内容推荐
相近分类:
推荐阅读





